Next Step in Care: Family Caregivers & Health Care Professionals Working Together
Guides & Checklists
- For Family Caregivers
- For Health Care Providers
- Para Cuidadores Familiares
-

- Для лиц, ответственных за медицинский уход
- Videos
- Links and Resources
- Terms and Definitions
- Quality Improvement Surveys
- News
- About Next Step in Care
- About United Hospital Fund


Frequently Asked Questions about Engaging Family Caregivers
The following questions are four of the most frequently asked related to engaging family caregivers:
1. Why are family caregivers important to transitions?
Despite the enormity of the American health care system, family caregivers are and will remain the primary source of care for their seriously and chronically ill (and often elderly) relatives and friends.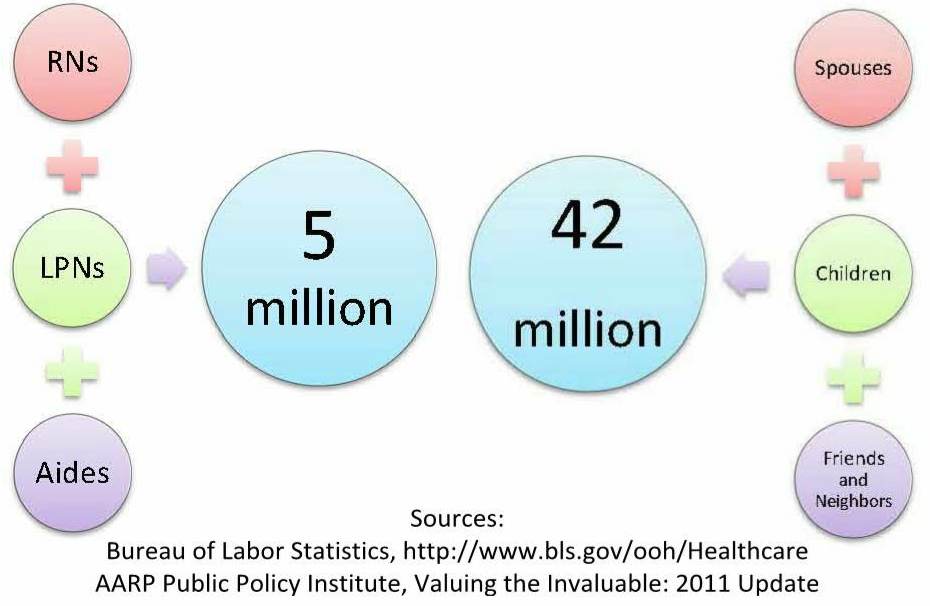
In today's fast-paced, technologically driven and financially constrained health care environment, untrained, unpaid, and unsupported family members have been expected to take on ever more daunting and long-term responsibilities. They are responsible for increasingly complex tasks including medication management, care coordination, and financial and legal assistance, in addition to the emotional support that is often the special province of long-standing family ties. For details on the medical and nursing tasks performed by many of today's family caregivers, see the AARP/United Hospital Fund report "Home Alone: Family Caregivers Providing Complex Chronic Care."
Incorporating family caregivers into care, from information gathering and medication reconciliation, to education and training, to discharge planning and post-discharge care, can be a critical component of your work to support frail and chronically ill patients.
For more, see How can I identify family caregivers?
For tools to help integrate family caregivers into transitions, see Toolkit.
2. How can I identify family caregivers? How are family caregivers different from persons with powers of attorney, next of kin, and other decision makers?
Few people live in a bubble. Most seriously and chronically ill people have someone who helps in some way. It could be a neighbor who knocks on the door every day and drops off the paper, and will pick up prescriptions if the patient is unwell. It could be a spouse who is giving injections because the patient’s hands shake. It could be several adult children: one does the shopping and cooking, another takes the patient to the doctor, and another handles the finances and insurance.
Family caregivers can be anyone who provides care as "family” (in the broadest sense of the term). As health care has changed, so has family caregiving, with more complex medication regimens, shorter stays in hospitals and rehabilitation centers, more skilled care done at home, and more people living with cognitive impairments and requiring continual supervision and redirection.
Many people do not identify themselves as “family caregivers,” and many patients do not identify themselves as needing caregiving. To find out who the family caregiver is, ask the patient about specific tasks. For example:
”When you go to the doctor, who goes with you, or arranges a ride?”
"If you don’t feel well, who do you call?” or “…who helps you out?”
“I want to make sure everyone knows about your new diet, because it’s very important for keeping you well. Who does most of the cooking in your house?”
If the patient is unable to answer or has impairments in cognition or judgment, ask next of kin or other emergency contacts. Remember that the person at a hospital bedside may simply be a visitor, and not someone who provides care. It is best not to make assumptions about who family caregivers should be, such as a spouse or adult child or a person living in the same home. Individual functions in care situations vary widely, even among groups that have strong traditional roles.
Once a family caregiver has been identified, speak with that person. The person may be able to handle the new caregiving responsibilities or may need training, assistance, or respite in order to continue. It's also possible that the person may not be able to continue. Having that conversation with the identified family caregiver can assist you in making a successful plan of care.
To learn how family caregiver identification was done by health care providers in TC-QuIC, see page 13 of the report.
3. If the patient is alert and oriented, why involve anyone else? Isn't that more work?
Recent studies have shown that even independent, cognitively intact adults retain less than half of the instructions they receive in the hospital. Essential information, such as changed medication regimens, follow-up appointments, and modified diets, can be misunderstood or lost. The patient may not be the person cooking or managing medications for the short term, or may never be responsible for these tasks within the household.
Educating and planning with the family caregiver who will be implementing the transition plan can be a more effective use of staff time and effort. Also, an informed, involved family caregiver can supplement and reinforce the patient's understanding, which may be reduced due to illness and the stress of the situation.
For more, see Why are family caregivers important to transitions?
For tools to help integrate the family caregiver into transitions, see the Toolkit.
4. What you DON'T know about HIPAA and family caregivers...
It's a common misconception that the HIPAA law prevents health care providers from speaking with family caregivers unless the patient has signed for permission, or unless the person has power of attorney, health care proxy, guardian, or other legal representational status.
While this may be a part of an organization's own protocols, it is NOT part of the HIPAA law.
What IS part of HIPAA, however, is that health care providers should use their own best judgment in working together with people who provide care to the patient or are responsible for the patient's health care bills. The only restriction is if the patient (or legal representative) specifically refuses.
For details, please see:
Family Caregivers’ Rights to Patient Information: What Health Care Providers Need to Know
U.S. Department of Health and Human Services Office for Civil Rights
Health Privacy Project at the Center for Democracy & Technology